
The sighting and monitoring of any new COVID-19 variant—this time it’s CH.1.1—must be given context, experts say.
Omicron subvariants XBB and XBB 1.5 caused concern among public policy officials when they first surfaced, as did BQ and BQ 1.1. That those four subvariants account for 95.9% of new cases of the virus in the U.S. for the week ending Feb. 3, according to the Centers for Disease Control and Prevention (CDC), proves that those concerns weren’t unfounded.
However, despite the new variants, the U.S. continues to move toward a place where it might finally consign the pandemic to history.
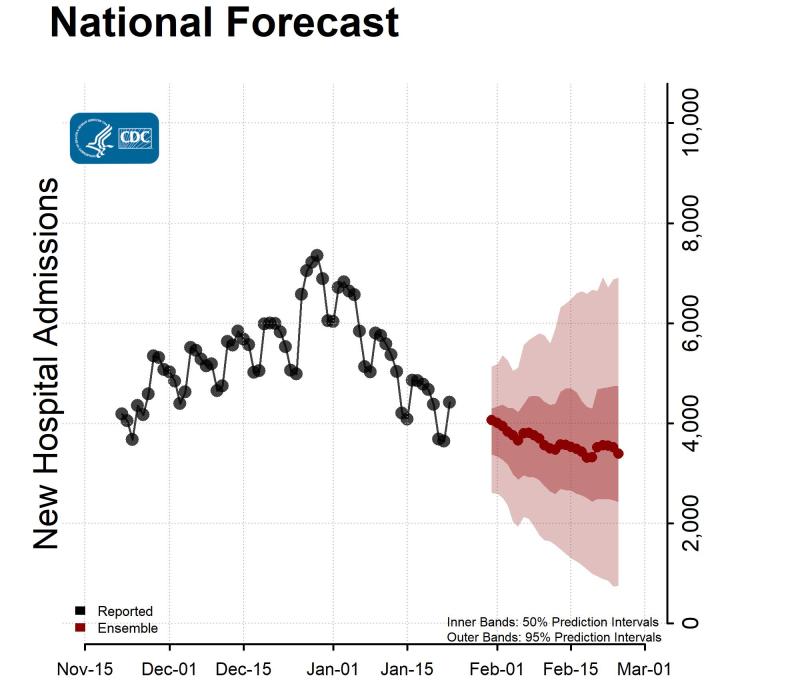
The approximately 479,000 new COVID-19 cases that the U.S. averaged a month ago has dropped to about 281,000 according to the CDC. The seven-day average hospital admissions stand at 3,919, compared to 4,279 a month ago.
The COVID-19 national emergency and public health emergency ends on May 11. Nonetheless, the CDC urged caution, as the agency no longer believes that COVID-19 hospitalizations will decrease over the next month with “6,900 new confirmed COVID-19 hospital admissions likely reported on February 24, 2023.”
A preprint paper released last week by researchers at Ohio State University says that CH.1.1 has “a consistently stronger neutralization resistance available than XBB, XBB.1 and XBB.1.5, which is astonishing and warrants continuous monitoring and further investigations.”
Their study notes that CH.1.1 contains the mutation L452R that’s seen in delta, but not in omicron, and this may give CH1.1 the ability to become more infectious than other omicron stains. CH.1.1 has been nicknamed Orthus, after the two-headed dog in Greek mythology.
CH1.1 now occupies 5th place on the list of spreading variants, accounting for 1.6% of total new cases in the U.S., according to the CDC.
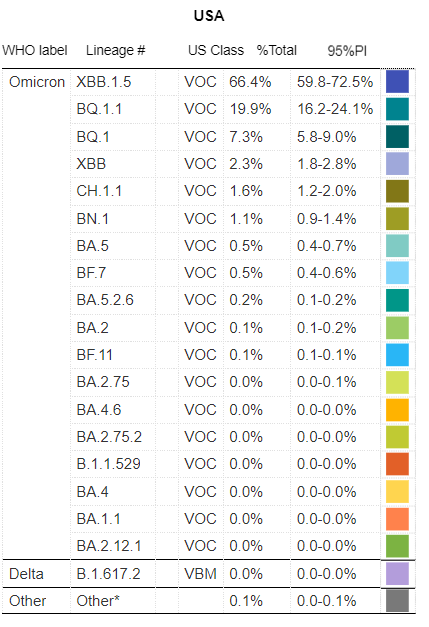
For instance, the BQ.1.1 variant—which now occupies 2nd place as a cause of new infections in the U.S., accounting for 19.9%—had flown under the radar for weeks before first emerging on the CDC’s list in October when it then accounted for just 2.4% of new cases.
CH 1.1 has made its presence known in the U.K., where it accounted for 28.2% of new sequence infections compared to XBB.1.5’s 10.9% of sequenced infections as of January 15, the most recent data available by that country’s Office of National Statistics.
Mary Ramsay, M.D., the head of immunization at the UK Health Security Agency, said in a press release that “it’s concerning that the recent downward trend in COVID-19 hospitalizations has started to show signs of a reverse this week.” Ramsay also said that “two variants, CH.1.1 and XBB.1.5, have a growth advantage in the UK and we can expect further increases in transmission and hospitalizations in future weeks.”
Ohio State researchers created CH.1.1 in a laboratory and tested it against blood taken from 14 healthcare workers who had gotten two and four doses of monovalent vaccine, as well as the bivalent vaccine aimed at omicron and its subvariants. The workers’ blood generated 17 times fewer antibodies against CH.1.1 as they did against BA.4 and BA.5, according to the study.